
According to the Centers for Disease Control and Prevention (CDC), 70% of adults between the ages of 40 and 79 used at least one prescription drug in the past 30 days in the United States, and approximately 20% took at least five prescription drugs.
Here are some common culprits for oral health problems linked to medications, as well as other drugs that can potentially cause the same issues, along with some suggestions on how to prevent and treat the conditions.
 1. Excessive bleeding during or after invasive procedures, like a tooth extraction or other oral surgery
1. Excessive bleeding during or after invasive procedures, like a tooth extraction or other oral surgery
Common culprits: Commonly prescribed blood thinners like warfarin (Coumadin), rivaroxaban (Xarelto) and apixaban (Eliquis). These drugs are often used by those who’ve recently undergone knee or hip replacement.
Other medications that may lead to excess bleeding: Antiplatelet meds such as Plavix is one common one. It is primarily used to prevent the recurrence of blood clots following a heart attack or stroke.
What to do: Inform your dentist of all of the medications you’re taking — including low-dose aspirin, which is often prescribed as a mild blood thinner, as well as any herbal supplements. Some herbal supplements can interfere with the metabolism of some of these drugs. Because it’s “herbal”, and not a “drug”, it may seem unrelated to you, but it may be very important, so be sure and tell them EVERYTHING you take.
Consult also with your primary care physician or specialist who prescribed the blood thinners to you. Depending on various factors, they may opt to have you stop taking them for a temporary period prior to having oral surgery to prevent excess bleeding. On the other hand, because of your individual circumstances and history, they may insist that you continue taking them, and be prepared for extended bleeding after your surgery. This is where we weigh the risks between dental and medical variables, and conclude which is best for you. Communication is the key here.
 2. Reduction of the pH level of saliva, causing the mineral structural breakdown of the teeth, and in time, causes cavities
2. Reduction of the pH level of saliva, causing the mineral structural breakdown of the teeth, and in time, causes cavities
 2. Reduction of the pH level of saliva, causing the mineral structural breakdown of the teeth, and in time, causes cavities
2. Reduction of the pH level of saliva, causing the mineral structural breakdown of the teeth, and in time, causes cavitiesMost common culprits: Gummy vitamins and other medications with added sugar.
Sugar is frequently an added ingredient in chewable vitamins and antacid tablets to make them more palatable (such as Tums) and in syrup-based concoctions (such as cough suppressants). Liquid antibiotics (liquid amoxicillin, for example, used by patients who have a hard time swallowing pills) may also contain sugar.
Particularly harmful, though, are the sticky gummy vitamins and other gummy supplements that stick onto and between your teeth, as well as long-lasting cough drops. These provide an acid bath for your teeth.
This is not good for your teeth — particularly if they are taken for a long period of time. Consuming sugar frequently reduces the pH level of saliva, causing it to become more acidic. Frequent pH drops in saliva causes a breakdown in the mineral structure of the tooth — and, over time, can cause cavities.
What to do: Ask your health care provider or pharmacist to see if there is a sugar-free alternative to your medication. If there is not, try and get yourself in the habit of brushing and flossing right after taking them.
Double down on your oral hygiene routine and use a fluoride mouth rinse to be certain you’re getting extra protection. Eat a diet low in sugar and starches. If you smoke – don’t. Take your medications with a meal. (Since you’re more likely to brush after eating, the sugar won’t linger on the tooth surfaces.) Be careful with the vitamin C. They often contain added sugar, and they can also increase the amount of acid in your stomach, which can lead to acid reflux, which can also lead to enamel erosion. Rinse your mouth after taking anything acidic. Baking soda is ideal, as it neutralizes the acid (Add 1 tsp to a glass of water and rinse and spit it out a few times).

3. Discolored teeth (yellow or brown stains) and increased tartar buildup
Common culprits: Some antibacterial oral rinses, like Chlorhexidine; antihistamines (like Benadryl); Anti-hypertension medications — including ACE inhibitors such as benazepril (Lotensin); Calcium channel blockers such as amlodipine (Norvasc) and felodipine (Plendil); and Beta-blockers such as metoprolol succinate (Lopressor) — all of which can reduce saliva production, making it harder to get rid of stain-causing debris in the mouth.
Cholesterol medication Cholestyramine (Prevalite), a powder-formulated med designed to be mixed in a beverage, can result in discoloration when sipped slowly.
Inhaled corticosteroids, such as fluticasone (Flonase), can also damage tooth enamel because of the acid content in the spray.
What to do: It’s important to distinguish the type of discoloration that your medications are causing.
Extrinsic discoloration on the surface of the tooth — from mouth rinses containing chlorhexidine, for example — can be cleaned off at your next dental hygiene visit or with a whitening treatment.
For deeper INtrinsic discoloration your dentist may recommend bonding, porcelain veneers or crowns.
4. Bulky, gingival (gum tissue) overgrowth
 4. Bulky, gingival (gum tissue) overgrowth
4. Bulky, gingival (gum tissue) overgrowthThis is a buildup of swollen gum tissue that begins to grow over the teeth, creating the perfect environment for bacteria. Not only is this unsightly, it can also lead to quite a bit of pain and discomfort if the overgrowth gets in the way of chewing.
Common culprits: High blood pressure medications such as amlodipine (Norvasc) and felodipine (Plendil) are frequent offenders. Other culprits include anti-seizure medications, such as phenytoin (Phenytek); and immunosuppressive agents, such as cyclosporine (Neoral and Gengraf) and methotrexate (Otrexup and Trexall).
This gingival tissue overgrowth doesn’t usually happen from the drugs alone. It’s usually the drug in combination with tissue irritation from things like plaque. With good oral hygiene, we don’t tend to see these problems.
What to do. Ask your doctor if there is an alternative medication that might work.
More frequent cleanings (every 3-4 months) should also help lower your chances of developing this condition. Patients who already have overgrowth should increase their oral hygiene regimen. It won’t reverse the problem, but plaque control can prevent it from getting worse.
If the problem becomes very severe, there are surgical procedures that can remove overgrown gum tissue. However, in some cases, this is a temporary fix because ongoing use of the medication will often lead to continued overgrowth, and over time the gum tissue will come back again.
Excellent, consistent, impeccable oral hygiene is the best defense here.
5. Osteonecrosis of the jaw (ONJ). A RARE, but potentially serious complication that causes death of the jawbone
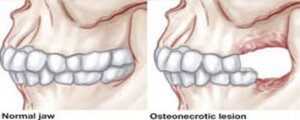 5. Osteonecrosis of the jaw (ONJ). A RARE, but potentially serious complication that causes death of the jawbone
5. Osteonecrosis of the jaw (ONJ). A RARE, but potentially serious complication that causes death of the jawboneCommon culprits: Osteoporosis and osteoarthritis bisphosphonates such as alendronate (Fosamax), risedronate (Actonel and Atelvia) and ibandronate (Boniva).
What to do: Talk to your doctor about potential alternatives to bisphosphonate drugs that may pose less risk. Before scheduling dental work, discuss your osteoporosis drug history with your surgeon and your doctor. The longer a patient is on this medication, the higher the risk is for ONJ. If you’ve been on it for several years, it may be necessary to stop taking it for 2-3 months prior to having major oral surgery in order to eliminate this risk, however small it might be. Proactive dental care before and during antiresorptive drug therapy can reduce the risk of developing ONJ by as much as 50 percent.
Keep it clean.
6. Dry mouth
 6. Dry mouth
6. Dry mouthDry mouth (also known as Xerostomia) is a serious and extremely common side effect of more drugs than we can name here.
It greatly increases the risk for cavities, gum disease and canker sores. Saliva not only lubricates the mouth, but it also neutralizes the acid produced in the mouth. As we age, our salivary glands become less active, making us more susceptible to tooth decay. Taking medications that exacerbate this problem only makes the effects worse.
Xerostomia/Dry mouth is a potential side effect of literally hundreds of medications that interrupt the production of saliva. In particular, drugs that alter our central nervous system.
Common culprits: Anxiety drugs anxiety meds such as escitalopram (Lexapro) and sertraline (Zoloft);, anti-depressants and antidepressants such as fluoxetine (Prozac) and alprazolam (Xanax); urinary & bladder medications to treat urinary incontinence or an overactive bladder, such as oxybutynin chloride (Ditropan XL) and oxybutynin (Oxytrol); Parkinson’s disease medications such as levodopa, also called L-dopa (Sinemet); blood pressure and heart medications, including ACE inhibitors such as lisinopril (Prinivil and Zestril), enalapril (Innovace) and benazepril (Lotensin); Beta-blockers such as metoprolol succinate (Lopressor and Toprol XL); Diuretics which help rid your body of water and salt to bring down blood pressure, such as furosemide (Lasix).
Radiation therapy and chemotherapy may also damage the salivary glands.
What to do: If this is a severe problem, perhaps the medication can be changed. If that isn’t possible, the patient needs a strategy to minimize symptoms. Discuss this with your dentist. There are protocols and products to help you manage this. Keep a bottle of water nearby and sip on it throughout the day to keep your mouth moisturized. (Consuming a lot of coffee or tea can make dry mouth worse). Try a mouthwash containing Xylitol; they’ve been shown to help promote saliva production). Try an over-the-counter saliva substitute like Allday Dry Mouth Spray, or perhaps a prescription from your dentist for one of the various dry mouth remedies. Use a humidifier, particularly at night, next to your bed if you are a mouth-breather.
It is also very likely you will need to be seen for more frequent cleanings and check-ups. This is because the rate and likelihood of recurring decay is a very real. Even for patients with immaculate homecare, this can be a problem. As of now, there is no cure, only diligent, consistent care, moisturization and attention to manage it.
7. Painful, soft-tissue reactions, including mucositis (inflammation of the mucous membrane that lines the inside of the mouth, and ulcerated sores inside the mouth or on the tongue)
 7. Painful, soft-tissue reactions, including mucositis (inflammation of the mucous membrane that lines the inside of the mouth, and ulcerated sores inside the mouth or on the tongue)
7. Painful, soft-tissue reactions, including mucositis (inflammation of the mucous membrane that lines the inside of the mouth, and ulcerated sores inside the mouth or on the tongue)Common culprits: NSAIDs such as ibuprofen and aspirin; hypoglycemic agents for type 2 diabetes such as metformin (Fortamet or Glucophage); beta-blockers, including metoprolol succinate (Toprol XL) and bisoprolol (Zebeta), used by those with angina, high blood pressure and abnormal heart rhythm to help the heart beat more slowly; and immunosuppressive agents, among them prednisone (Deltasone) and methotrexate (Otrexup and Trexall), which are commonly taken by people with autoimmune diseases such as rheumatoid arthritis, multiple sclerosis and inflammatory bowel disease.
Chemotherapy and radiation therapy may also cause changes in the lining of the mouth and the salivary glands. This can upset the healthy balance of bacteria. Quick-dissolving tablets that dissolve under, or on top of your tongue like nitroglycerine tablets (Nitrostat) used to prevent angina (chest pain) caused by coronary artery disease, anti-nausea medications such as ondansetron (Zofran), or benzodiazepines such as lorazepam (Ativan), which target anxiety or sleeping problems can cause irritation at the site.
What to do:
- Keep your mouth clean and see your dentist regularly.
- Beware of toothpastes with anti-plaque or anti-tartar ingredients, as they sometimes cause adverse reactions in some people experiencing these symptoms.
- Avoid hot, salty or spicy foods until your mouth heals.
- Avoid hard, sharp munchies (like chips or crackers) and stick with softer, moist foods.
- Steer clear of alcohol, and acidic juices.
- Don’t smoke: the heat and chemicals in tobacco irritate the mucous membranes.
- To help with inflammation and discomfort, try gently sucking on ice, allowing the ice chips to slowly dissolve in your mouth.
- Try a soothing homemade mouth rinse by mixing a teaspoon of baking soda and a teaspoon of salt in 4 cups of warm water. Swish the solution around in your mouth, then spit it out. Keep the remaining solution in a covered container at room temperature and use throughout the day. (Bonus: It helps keep the inflamed tissue clean.)
- Your dentist may also prescribe a rinse or some other anesthetic, antifungal or antibiotic med to coat the tissues.





