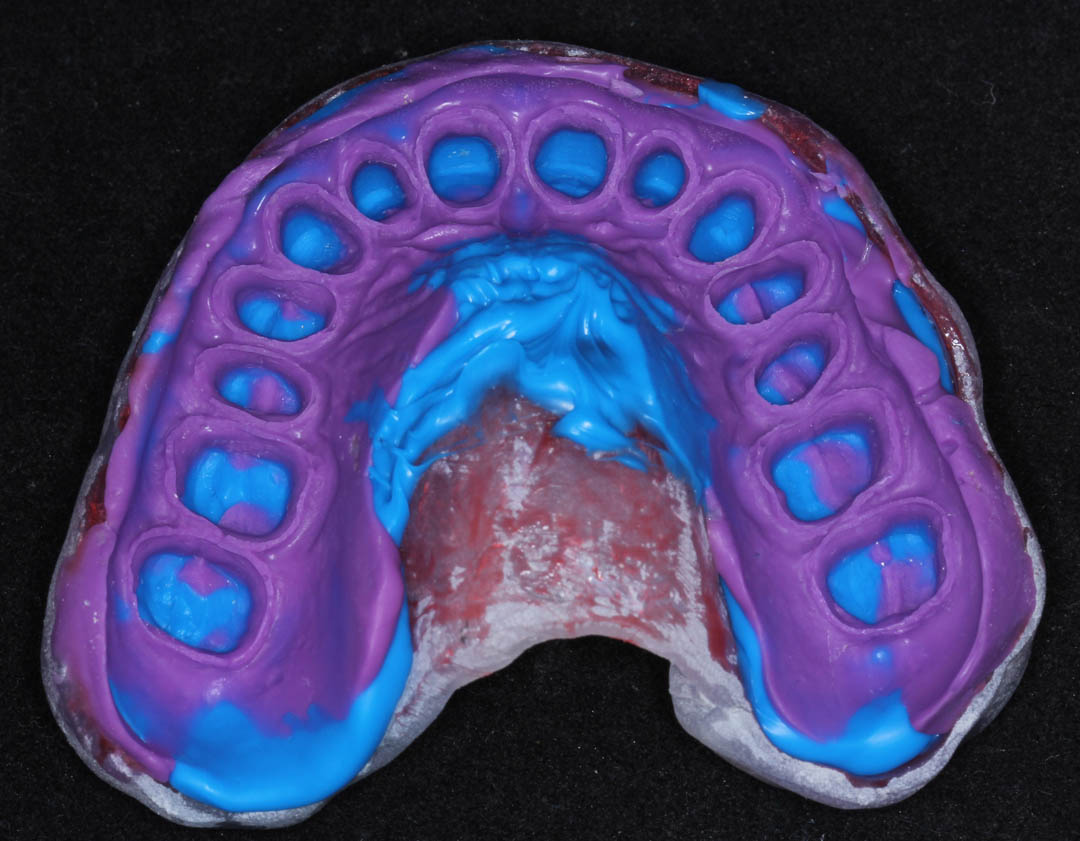
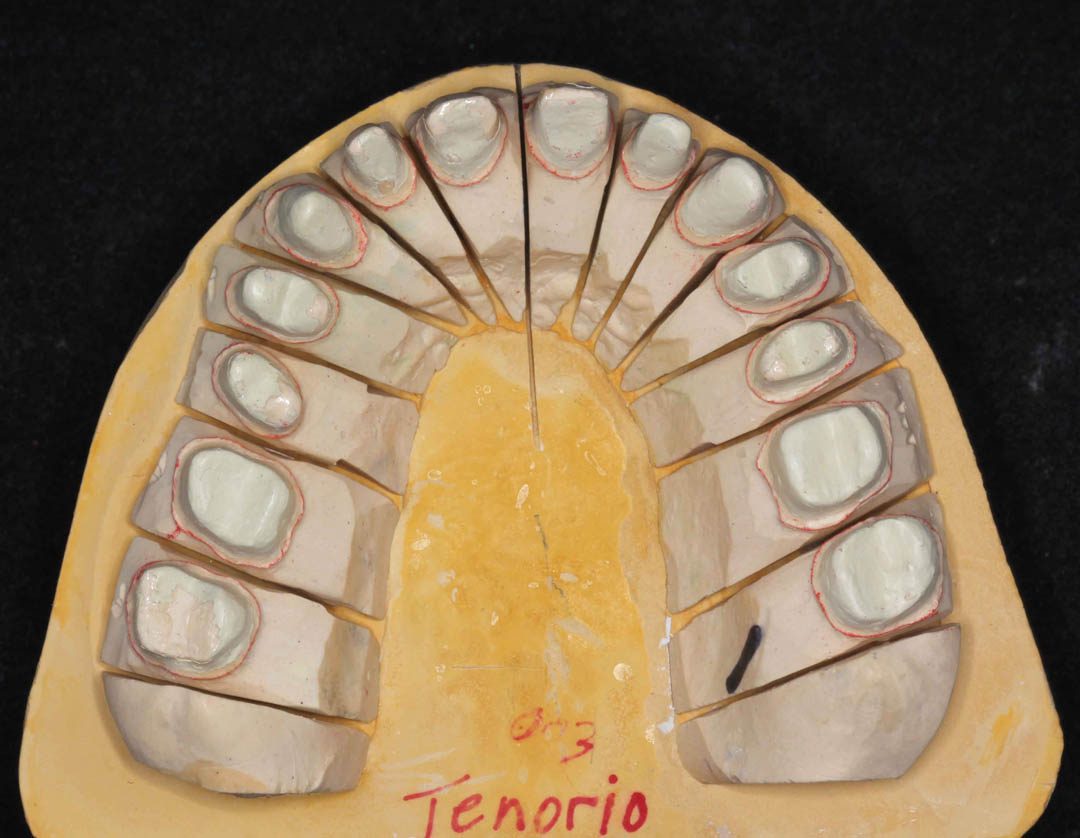
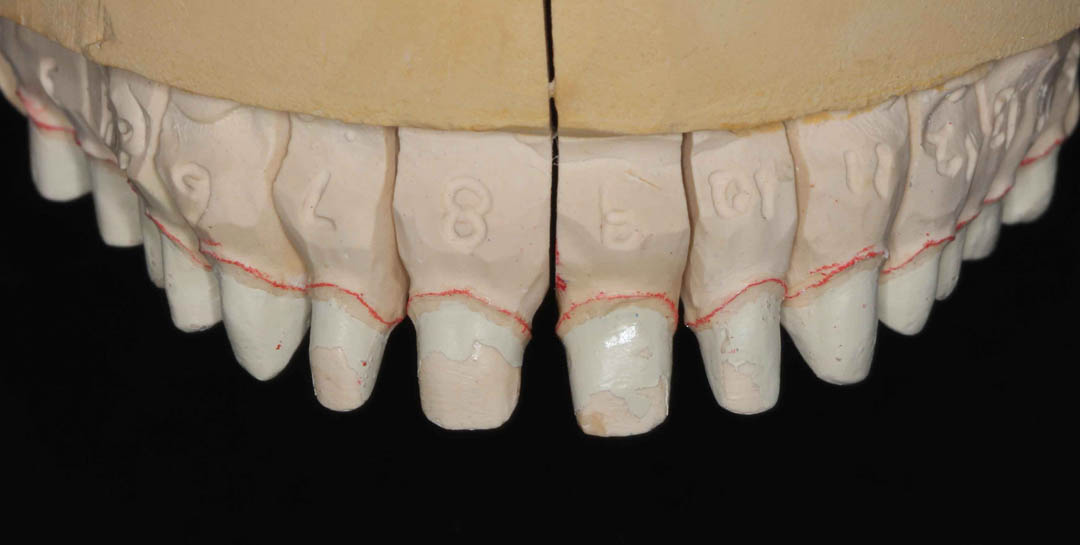
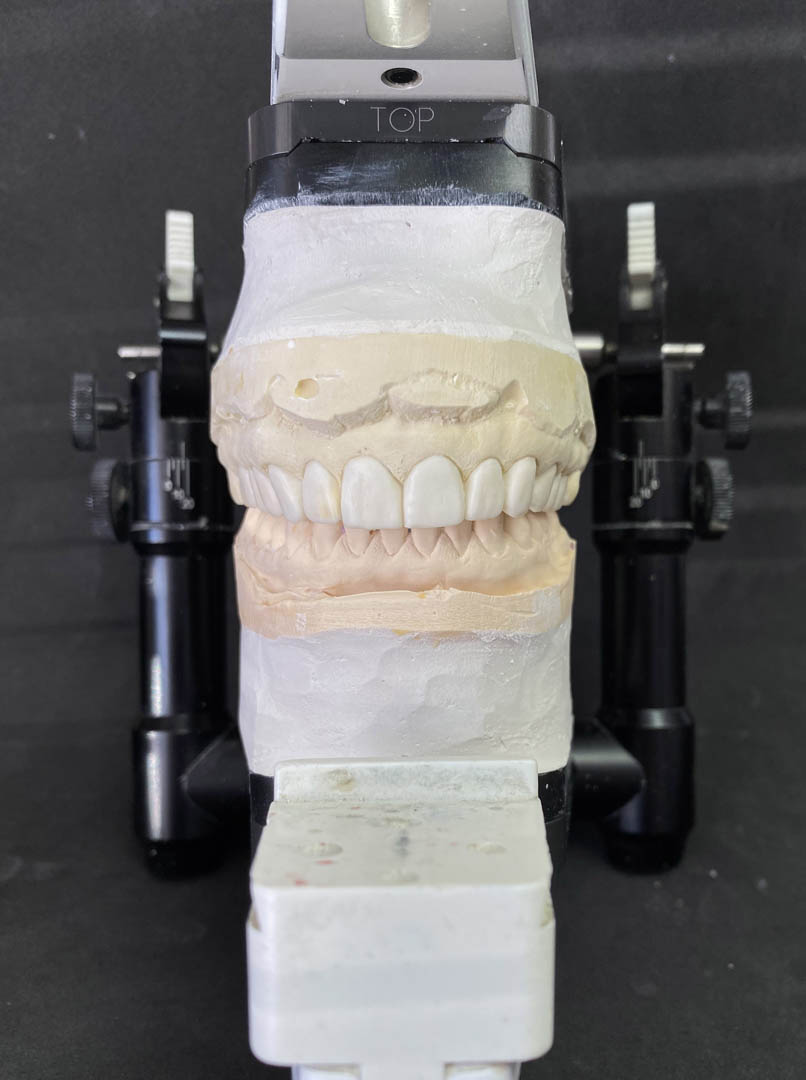
After two months of healing, a “final impression” is made. THIS IS THE MOST DIFFICULT PROCEDURE IN DENTISTRY and most dentist simply cannot do it. Why is it difficult? Preparing 14 teeth, protecting the gums, retracting the gums, prevent bleeding, control material, keep patient comfortable. Less than 5% of dentists can do all the above. Note that every spec of the margin of all 14 crowns are represented in this impression. This is not an exaggeration… 5%.