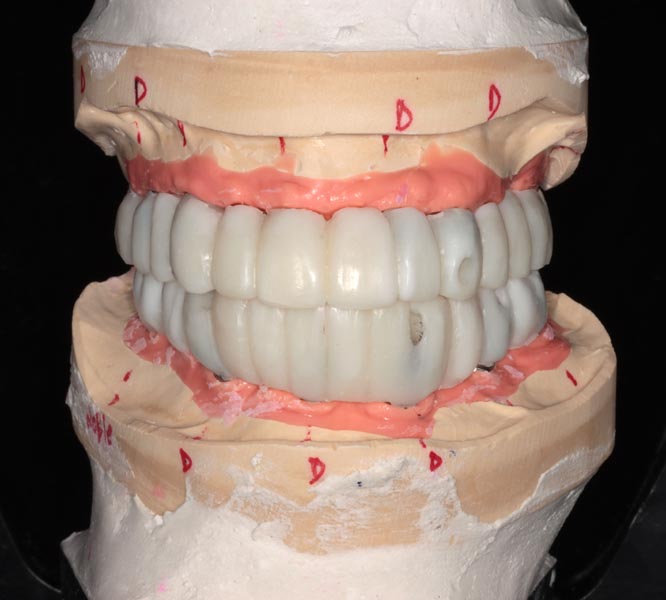
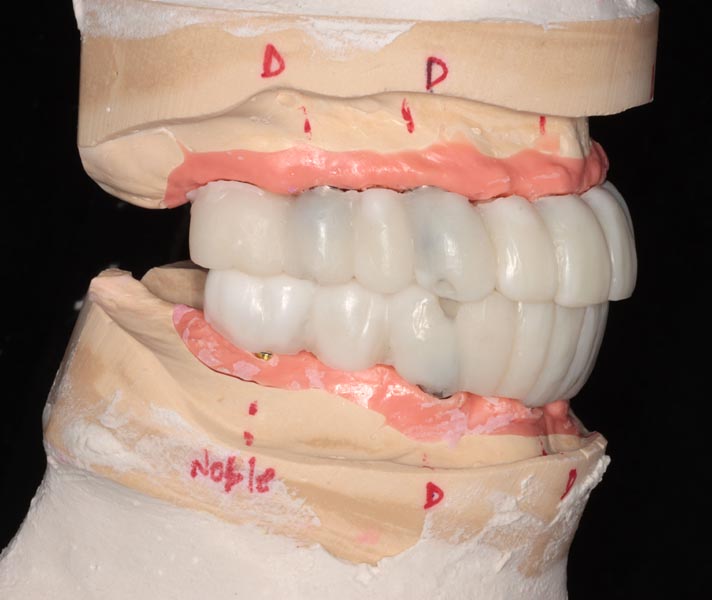
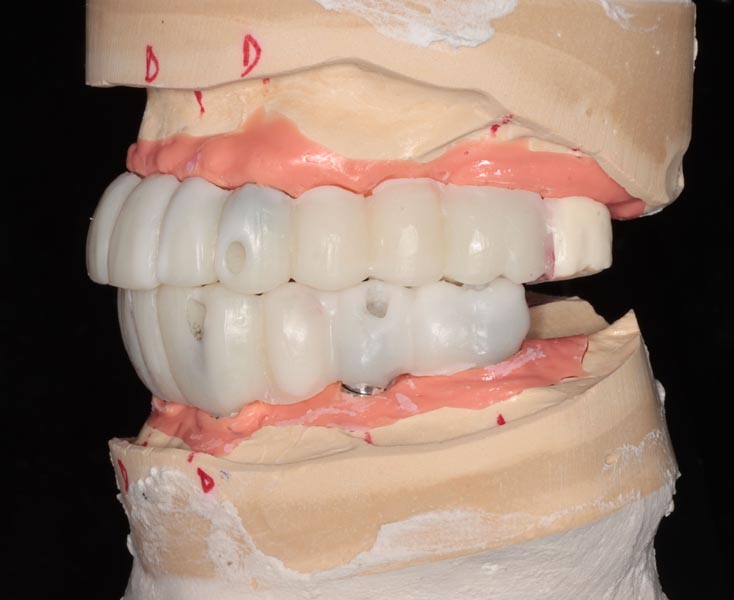
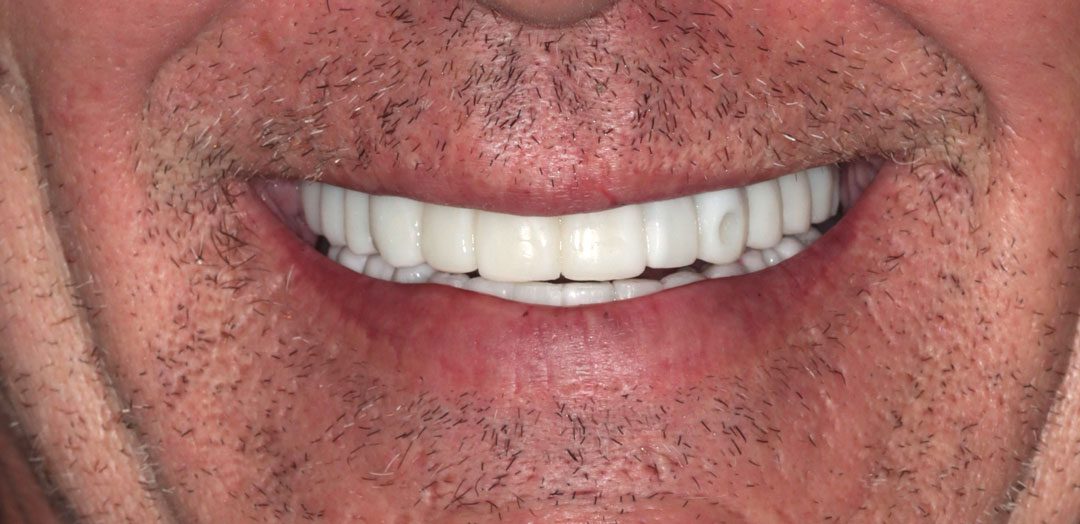
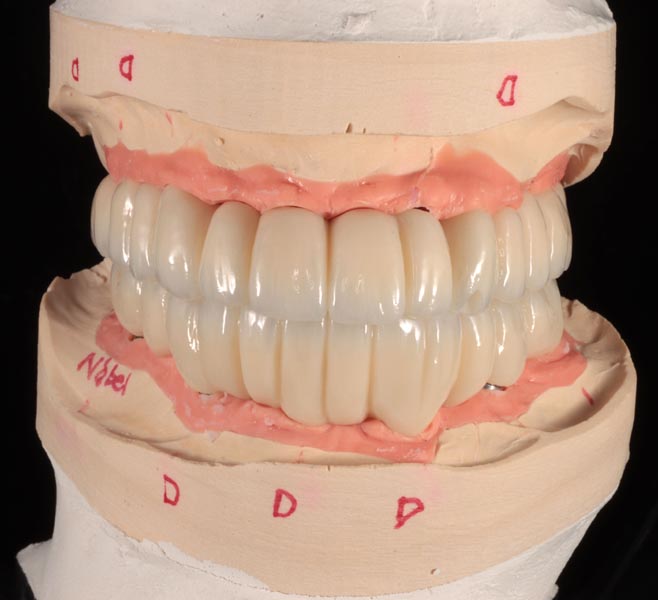
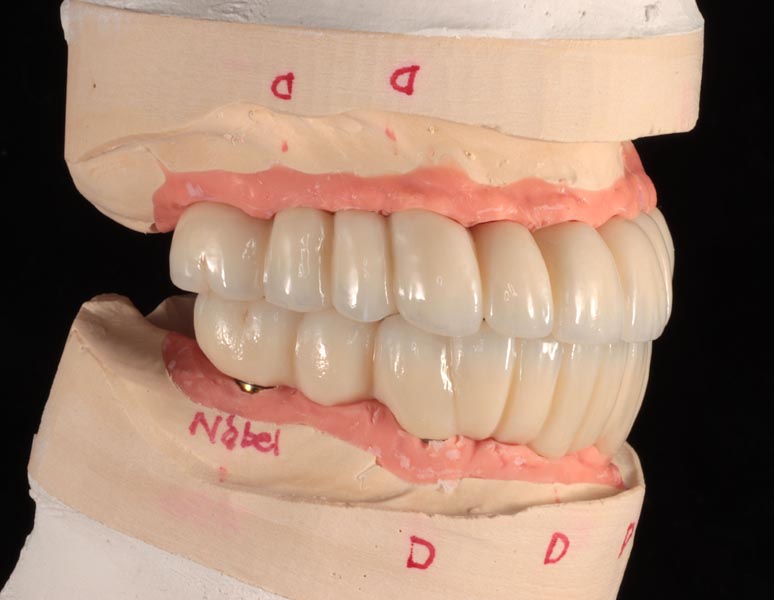
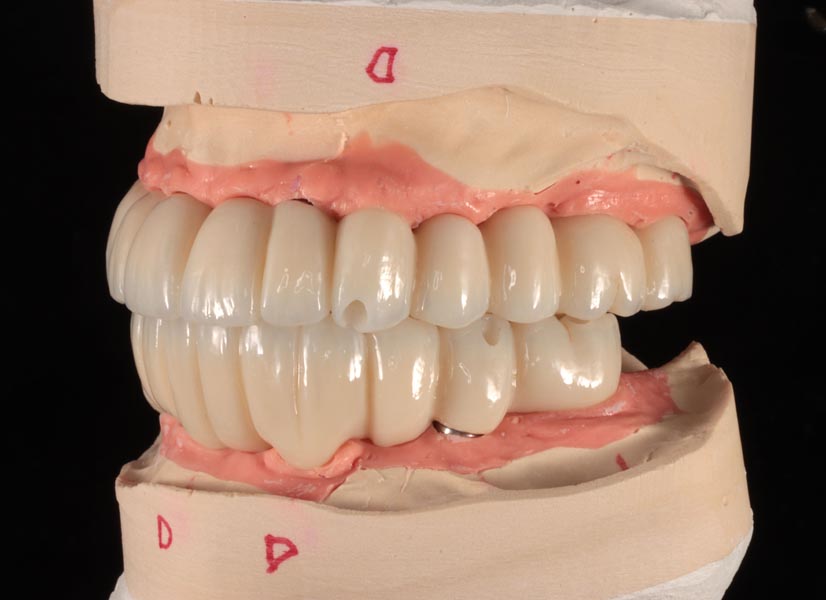
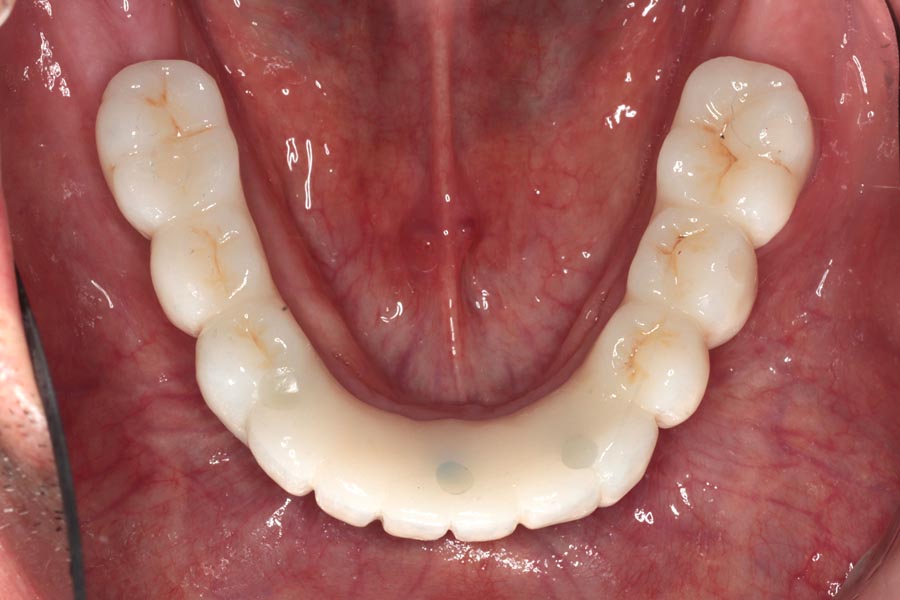
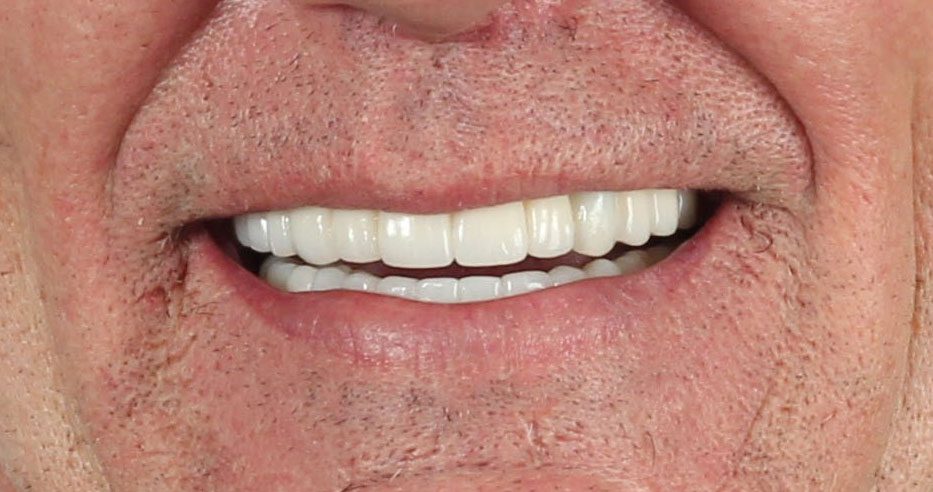
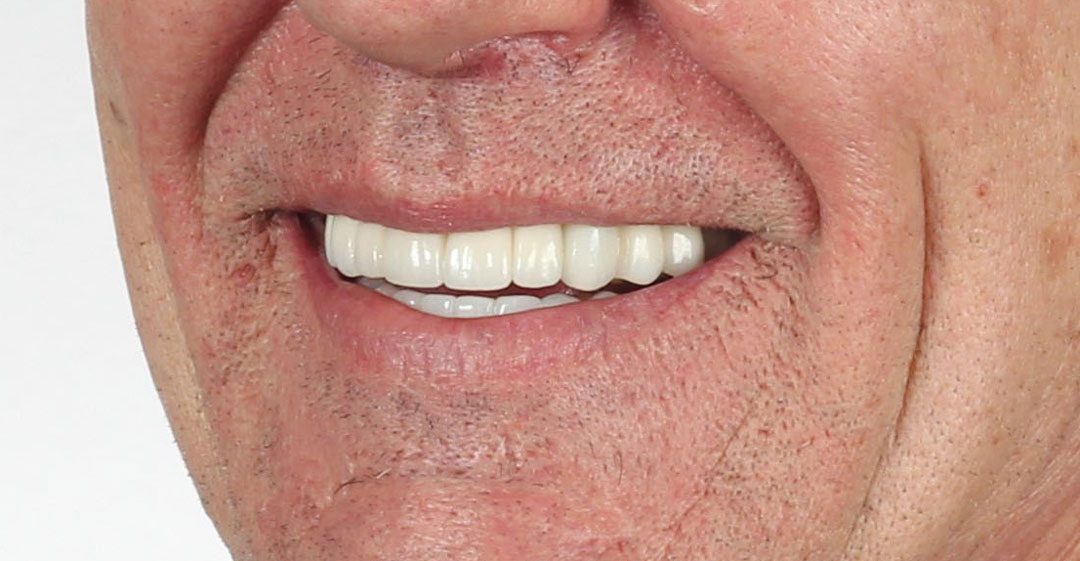
Final, zirconia prostheses – frontal view. The lab then uses the wax prototypes to fabricate definitive zirconia prostheses. These restorations are hand-finished by a team of talented dental technicians to ensure a beautiful, life-like result. The teeth are characterized, producing different zones of translucency and opacity, as opposed to making them look like a single monochromatic block. In this particular case, some of the implants’ trajectories were angled too steeply to correct, even with special angle-correcting screws. We had to overcome this by having the screw access holes come out from the front of the tooth and sealing them after with a tooth-colored filling material.























 (Female)")